-
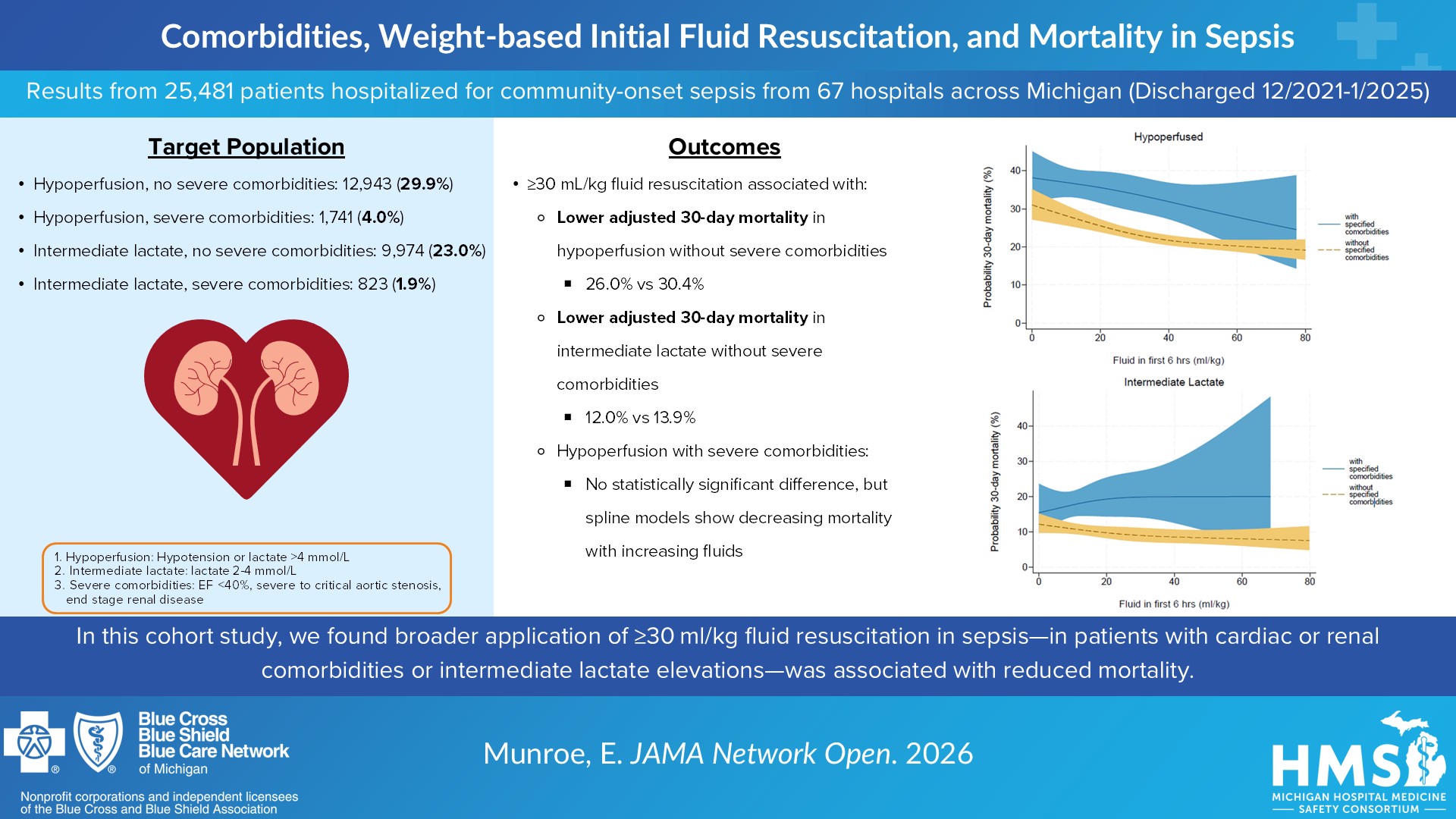
Comorbidities, Weight-Based Initial Fluid Resuscitation, and Mortality in Patients With Sepsis
In this cohort study of patients with community-onset sepsis, initial administration of 30 mL/kg or more of fluid was associated with lower 30-day mortality among patients who had either hypoperfusion or intermediate lactate elevation without severe cardiac or kidney comorbidities. The findings suggest that broader application of at least 30 mL/kg of initial fluid resuscitation for sepsis in patients with hypoperfusion and cardiac or kidney comorbidities or intermediate lactate elevation may reduce sepsis-related mortality.
Download the Visual Abstract -
Timely Antibiotics and Fluid Resuscitation Are Associated With Increased Discharge to Home After Sepsis
Our results show that in this multihospital cohort, timely antibiotic delivery and fluid resuscitation were associated with increased discharge to home after sepsis. This finding suggests that timely treatment of sepsis may reduce downstream morbidity and health care expenditures.
Download the Visual Abstract -
CDC’s Hospital Sepsis Program Core Elements are associated with improved management and outcomes of sepsis
In this multi-hospital cohort, we found that robust hospital sepsis programs—as measured by a summary Core Elements Score—were associated with guideline-concordant management and lower risk-adjusted mortality in patients hospitalized for sepsis. Furthermore, the Core Elements Score was independently associated with management and outcomes of sepsis after adjustment for hospital characteristics. These findings suggest that robust hospital sepsis programs can improve the management and outcomes of sepsis.
Download the Visual Abstract -
Antibiotic De-Escalation in Adults Hospitalized for Community-Onset Sepsis
In this study, de-escalation of empiric broad-spectrum antibiotics (BSA) therapy at day 4 was associated with similar safety outcomes, fewer antibiotic days, and shorter length of hospitalization among patients with community-onset sepsis compared with those who continued BSA therapy but varied widely in practice.
Download the Visual Abstract -
Goals of Care Assessment during Hospitalization for Sepsis
Sepsis is a common cause of hospital mortality, as well as new morbidity among survivors. Clinical practice guidelines recommend assessing goals of care (GoCs) during sepsis hospitalization to ensure goal-concordant care is provided. GoC assessment did not occur consistently during sepsis hospitalization in this multihospital cohort, even among higher-risk patients, and there was marked variation in practice across hospitals. Future work is needed to better understand what drives high performance in assessing GoC.
Download the Visual Abstract -
Epidemiologic Characteristics and Management of Sepsis Among Previously Healthy Patients
Most deaths resulting from sepsis occur among patients with advanced age, multiple morbidities, or frailty. It is unclear how many sepsis-related deaths truly are preventable. Previously healthy patients may provide insight into preventable sepsis mortality. We found that 1 in 10 patients with community-onset sepsis was healthy previously. Although gaps in in-hospital management were identified, deaths among previously healthy patients generally were deemed unpreventable with better in-hospital management because of patients seeking treatment too late in the course of sepsis. This study highlights system-level opportunities for better recognition and triage of sepsis before hospitalization.
Download the Visual Abstract -
Development and Validation of the Hospital Medicine Safety Sepsis Initiative Mortality Model
When comparing outcomes after sepsis, it is essential to account for patient case mix to make fair comparisons. We developed a model to assess risk-adjusted 30-day mortality in the Michigan Hospital Medicine Safety sepsis initiative (HMS-Sepsis). The HMS-Sepsis mortality model showed strong discrimination and adequate calibration and reclassified one-third of hospitals to a different performance category from unadjusted mortality. Based on its strong performance, the HMS-Sepsis mortality model may aid in fair hospital benchmarking, assessment of temporal changes, and observational causal inference analysis.
Download the Visual Abstract -
Institutional Structures and Processes to Support Sepsis Care: A Multihospital Study
To identify opportunities for improving hospital-based sepsis care and to inform an ongoing statewide quality improvement initiative in Michigan. Most hospitals used audit/feedback, order sets, and clinician education to facilitate sepsis care. Hospitals did not consistently incorporate organ dysfunction criteria into sepsis definitions. Existing processes focused on early recognition and treatment rather than recovery-based practices.
Download the Visual Abstract -
Use and Outcomes of Peripheral Vasopressors in Early Sepsis-Induced Hypotension Across Michigan Hospitals
Vasopressors traditionally are administered via central access, but newer data suggest that peripheral administration may be safe and may avoid delays and complications associated with central line placement. Peripheral vasopressor initiation was common across Michigan hospitals and had practical benefits, including expedited vasopressor administration and avoidance of central line placement in one-third of patients. However, the findings of wide practice variation that was not explained by patient case mix and lower use of first-line norepinephrine with peripheral administration suggest that additional standardization may be needed.
Download the Visual Abstract -
Hospital Policies on Intravenous Vasopressor Administration and Monitoring: A Survey of Michigan Hospitals
Overall, the variability in hospital policies suggests wide variation in practice. Hospitals should consider updating policies to permit peripheral vasopressors in scenarios in which their use has been shown to be safe: for short periods or longer durations with the use of multifaceted safety protocols.
Download the Visual Abstract -
Concordance of 30-Day Mortality and In-Hospital Mortality or Hospice Discharge After Sepsis
Sepsis contributes to 1.7 million adult hospitalizations and 350,000 deaths annually in the United States. To encourage improvements in sepsis management and outcomes, the Centers for Disease Control and Prevention (CDC) and the Centers for Medicare & Medicaid Services (CMS) are developing a risk-adjusted outcome measure for community-onset sepsis hospitalizations. Two candidate measures are (1) 30-day mortality after admission and (2) a composite outcome of in-hospital mortality or hospice discharge. While often preferred, 30-day mortality has drawbacks because post discharge vital status data are not available in real time, causing a lag in outcomes assessment. Furthermore, 30-day mortality measures used in CMS programs rely on claims and social security data available only for Medicare and Medicaid beneficiaries, thus limiting the eligible population. To inform decision-making about which measure to implement for national benchmarking, we evaluated the 2 candidate measures in a multihospital cohort.
Download the Visual Abstract

{kind=link}
{kind=link}
{kind=link}