
-
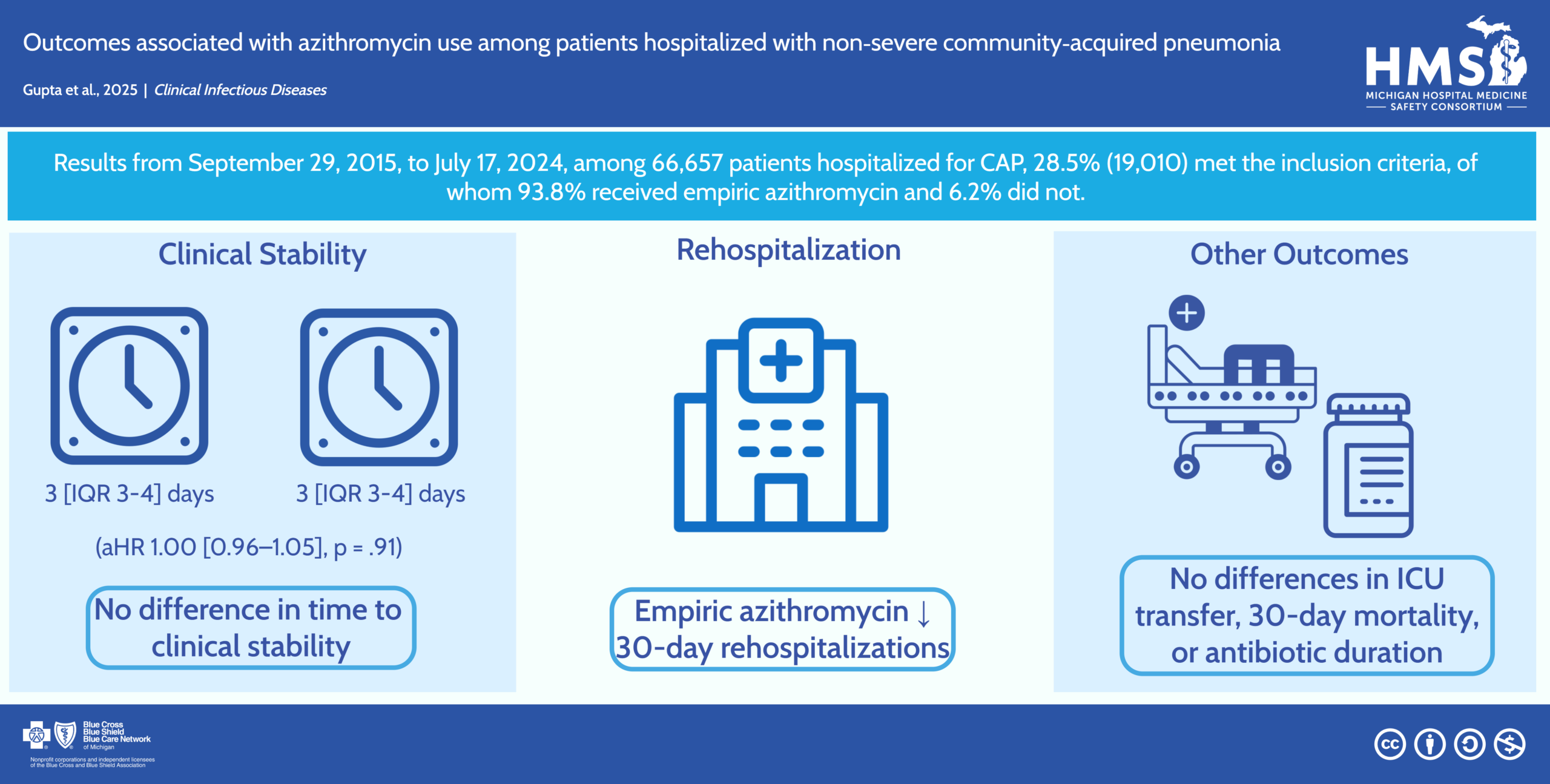
Outcomes Associated with Azithromycin Use Among Patients Hospitalized with Non-Severe Community-Acquired Pneumonia
Adding azithromycin to beta-lactam therapy in patients hospitalized with non-severe CAP was not associated with time to clinical stability but was associated with lower composite 30-day mortality and rehospitalization.
Download the Visual Abstract -
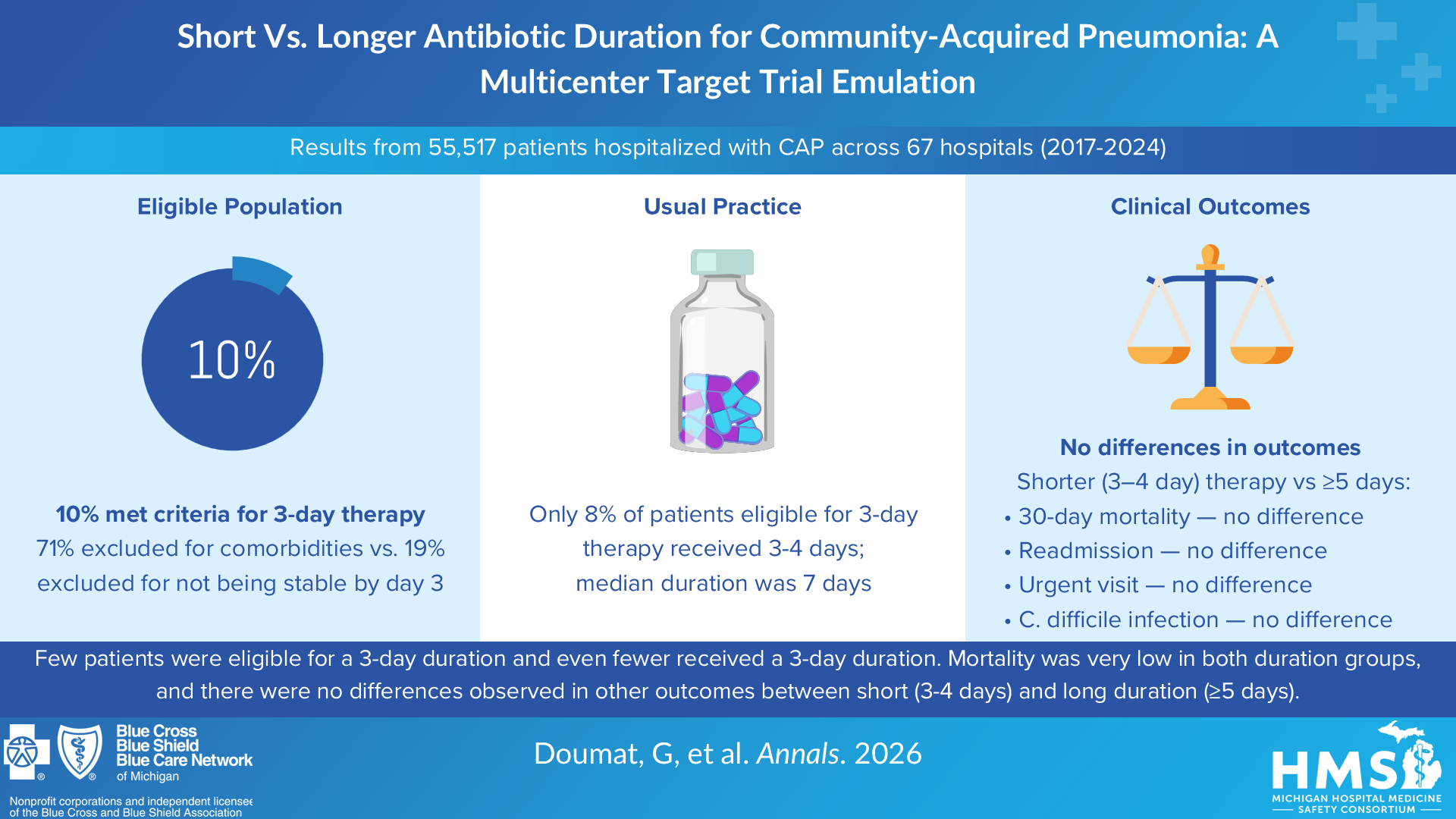
Short Versus Longer Antibiotic Duration for Community-Acquired Pneumonia: A Multicenter Target Trial Emulation
Among 55 517 hospitalized patients with CAP, 5620 (10.1%) ultimately met eligibility criteria for short-course therapy after comorbidity, clinical stability, and treatment duration criteria were applied. Median age of eligible patients was 68.2 years, and 54.3% were men. Median antibiotic duration was 7 days, with only 7.9% (444 of 5620) receiving 3 to 4 days. Thirty-day adjusted risk ratios for short- versus long-course antibiotic therapy were 0.89 for mortality (95% CI, 0.01 to 2.25), 1.07 for readmission (CI, 0.81 to 1.42), 0.94 for urgent visit (CI, 0.70 to 1.28), and 1.01 for C difficile infection (CI, 0.18 to 5.68). Only 10.1% of inpatients with CAP met the strict eligibility criteria for short-course therapy. The short- and longer-course antibiotic treatment groups had similar mortality rates, and there was little difference in benefits and harms.
Download the Visual Abstract -
Developing an approach to enhance recruitment for a cluster-randomised implementation trial: leveraging deliberative participation and credible messengers
We demonstrated the feasibility and impact of a novel approach to recruit hospitals from an existing collaborative to a cluster RCT using the principles of deliberative participation and credible messengers. While the approach was time-consuming, we achieved success at over-recruiting hospitals in a relatively short period of time. Strategies presented here may assist future trial organisers in implementing hospital-based cluster RCTs.
Download the Visual Abstract -
Target Trial Emulation of Empiric Antibiotics on Clinical Outcomes in Moderately Immunocompromised Patients Hospitalized with Pneumonia
Immunocompromised patients are often excluded from pneumonia trials, guidelines, and stewardship interventions. The objective of this study was to evaluate whether empiric broad-spectrum antibiotic treatment impacts mortality and other clinical outcomes in moderately immunocompromised patients without risk factors for multidrug-resistant organisms hospitalized with community-acquired pneumonia. Immunocompromised patients hospitalized with pneumonia often receive empiric broad-spectrum antibiotics despite low rates of multidrug-resistant organisms. Empiric broad-spectrum antibiotic use was not associated with mortality, but was associated with harm, including 30-day readmission, transfer to ICU and longer duration of hospitalization.
Download the Visual Abstract -
Community-Acquired Pneumonia: A Review
Community-acquired pneumonia (CAP) results in approximately 1.4 million emergency department visits, 740,000 hospitalizations, and 41,000 deaths in the US annually. Community-acquired pneumonia is common and may result in sepsis, acute respiratory distress syndrome, or death. First-line therapy varies by disease severity and etiology. Hospitalized patients with suspected bacterial CAP and without risk factors for resistant bacteria can be treated with β-lactam/macrolide combination therapy, such as ceftriaxone combined with azithromycin, for a minimum of 3 days.
Download the Visual Abstract -
Inappropriate Diagnosis of Pneumonia Among Hospitalized Adults
Little is known about incidence of, risk factors for, and harms associated with inappropriate diagnosis of community-acquired pneumonia (CAP). In this cohort study, inappropriate diagnosis of CAP among hospitalized adults was common, particularly among older adults, those with dementia, and those presenting with altered mental status. Full-course antibiotic treatment of those inappropriately diagnosed with CAP may be harmful.
Download the Visual Abstract -
Bacteremia From a Presumed Urinary Source in Hospitalized Adults With Asymptomatic Bacteriuria
Guidelines recommend withholding antibiotics in asymptomatic bacteriuria (ASB), including among patients with altered mental status (AMS) and no systemic signs of infection. However, ASB treatment remains common. In patients with ASB, bacteremia from a presumed urinary source was rare, occurring in less than 1% of patients with AMS. A personalized, risk-based approach to empiric therapy could decrease unnecessary ASB treatment.
Download the Visual Abstract -
A Statewide Quality Initiative to Reduce Unnecessary Antibiotic Treatment of Asymptomatic Bacteriuria
Hospitalized patients with asymptomatic bacteriuria (ASB) often receive unnecessary antibiotic treatment, which increases antibiotic resistance and adverse events. This quality improvement study showed that over 3 years, ASB-related antibiotic use decreased and was associated with a decline in unnecessary urine cultures. Hospitals should prioritize reducing unnecessary urine cultures (i.e., diagnostic stewardship) to reduce antibiotic treatment related to ASB.
Download the Visual Abstract -
Overdiagnosis of urinary tract infection linked to overdiagnosis of pneumonia: a multihospital cohort study
Reducing overdiagnosis of these two common infections may benefit from systematic interventions.
Download the Visual Abstract -
A Statewide Collaborative Quality Initiative to Improve Antibiotic Duration and Outcomes in Patients Hospitalized With Uncomplicated Community-Acquired Pneumonia
Community-acquired pneumonia (CAP) is a common cause for hospitalization and antibiotic overuse. We aimed to improve antibiotic duration for CAP across 41 hospitals participating in the Michigan Hospital Medicine Safety Consortium (HMS). Across diverse hospitals, HMS participation was associated with more appropriate use of short-course therapy and fewer adverse events in hospitalized patients with uncomplicated CAP. Establishment of national or regional collaborative quality initiatives with data collection and benchmarking, sharing of best practices, and pay-for-performance incentives may improve antibiotic use and outcomes for patients hospitalized with uncomplicated CAP.
Download the Visual Abstract -
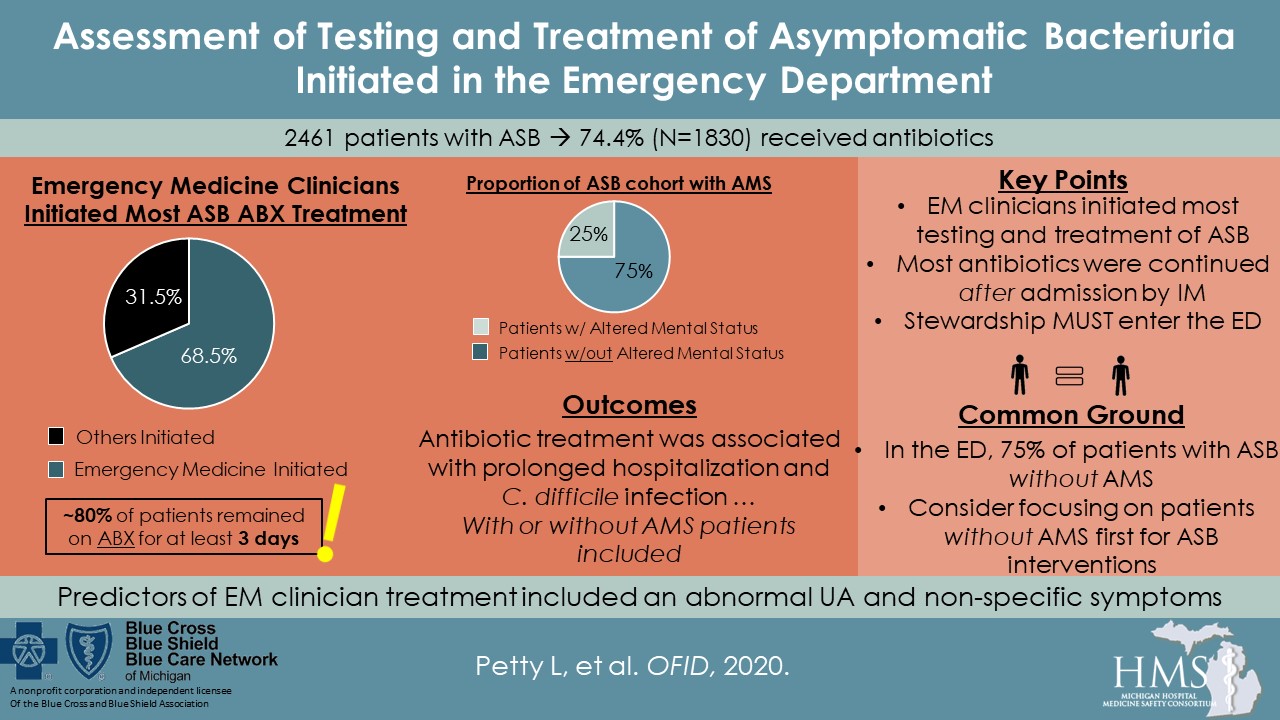
Assessment of Testing and Treatment of Asymptomatic Bacteriuria Initiated in the Emergency Department
Reducing antibiotic use in patients with asymptomatic bacteriuria (ASB) has been inpatient focused. However, testing and treatment is often started in the emergency department (ED). Thus, for hospitalized patients with ASB, we sought to identify patterns of testing and treatment initiated by emergency medicine (EM) clinicians and the association of treatment with outcomes. Among hospitalized patients ultimately diagnosed with ASB, EM clinicians commonly initiated testing and treatment; most antibiotics were continued by inpatient clinicians. Antibiotic treatment was not associated with improved outcomes, whereas it was associated with prolonged hospitalization and CDI. For best impact, stewardship interventions must expand to the ED.
Download the Visual Abstract -
Antibiotic Overuse After Hospital Discharge: A Multi-hospital Cohort Study
Antibiotics are commonly prescribed to patients as they leave the hospital. We aimed to create a comprehensive metric to characterize antibiotic overuse after discharge among hospitalized patients treated for pneumonia or urinary tract infection (UTI), and to determine whether overuse varied across hospitals and conditions. Antibiotic overuse after discharge was common and varied widely between hospitals. Antibiotic overuse after discharge was associated between conditions, suggesting that the prescribing culture, physician behavior, or organizational processes contribute to overprescribing at discharge. Multifaceted efforts focusing on all 3 types of overuse and multiple conditions should be considered to improve antibiotic prescribing at discharge.
Download the Visual Abstract -
Association of Infectious Disease Physician Approval of Peripherally Inserted Central Catheter With Appropriateness and Complications
Peripherally inserted central catheters (PICCs) are frequently used to deliver intravenous antimicrobial therapy. However, inappropriate PICC use may lead to patient harm. This cohort study suggests that, when PICCs were placed for intravenous antimicrobial therapy, infectious disease physician approval of PICC insertion was associated with more appropriate device use and fewer complications. Policies aimed at ensuring infectious disease physician approval prior to PICC placement for antimicrobials may improve patient safety.
Download the Visual Abstract -
A Deeper Dive Into Antibiotic Stewardship Needs: A Multihospital Survey
In a 2016 survey of 46 Michigan hospitals, we identified four key needs for antibiotic stewardship: clinically-relevant antibiotic data, monitoring compliance, syndrome-specific interventions, and discharge stewardship. A stewardship initiative now addresses these needs within the Michigan Hospital Medicine Safety Consortium.
Download the Visual Abstract -
Risk Factors and Outcomes Associated With Treatment of Asymptomatic Bacteriuria in Hospitalized Patients
Treatment of asymptomatic bacteriuria (ASB) with antibiotics is a common factor in inappropriate antibiotic use, but risk factors and outcomes associated with treatment of ASB in hospitalized patients are not well defined. Hospitalized patients with ASB commonly receive inappropriate antibiotic therapy. Antibiotic treatment did not appear to be associated with improved outcomes; rather, treatment may be associated with longer duration of hospitalization after urine testing. To possibly reduce inappropriate antibiotic use, stewardship efforts should focus on improving urine testing practices and management strategies for elderly patients with altered mental status.
Download the Visual Abstract -
Excess Antibiotic Treatment Duration and Adverse Events in Patients Hospitalized With Pneumonia: A Multihospital Cohort Study
Randomized trials demonstrate no benefit from antibiotic treatment exceeding the shortest effective duration. Patients hospitalized with pneumonia often receive excess antibiotic therapy. Excess antibiotic treatment was associated with patient-reported adverse events. Future interventions should focus on whether reducing excess treatment and improving documentation at discharge improves outcomes.
Download the Visual Abstract -
The Association of Antibiotic Stewardship With Fluoroquinolone Prescribing in Michigan Hospitals: A Multi-hospital Cohort Study
Fluoroquinolones increase the risk of Clostridioides difficile infection and antibiotic resistance. Hospitals often use pre-prescription approval or prospective audit and feedback to target fluoroquinolone prescribing. Whether these strategies impact aggregate fluoroquinolone use is unknown. Hospital-based stewardship interventions targeting fluoroquinolone prescribing were associated with less fluoroquinolone prescribing during hospitalization, but not at discharge. To limit aggregate fluoroquinolone exposure, stewardship programs should target both inpatient and discharge prescribing.
Download the Visual Abstract
Visual Abstracts
The aim of the antimicrobial use initiative is to formally measure and improve the appropriate use of antibiotics including selection of the right antibiotic for the right clinical condition for the right duration.
{kind=link}
{kind=link}
{kind=link}